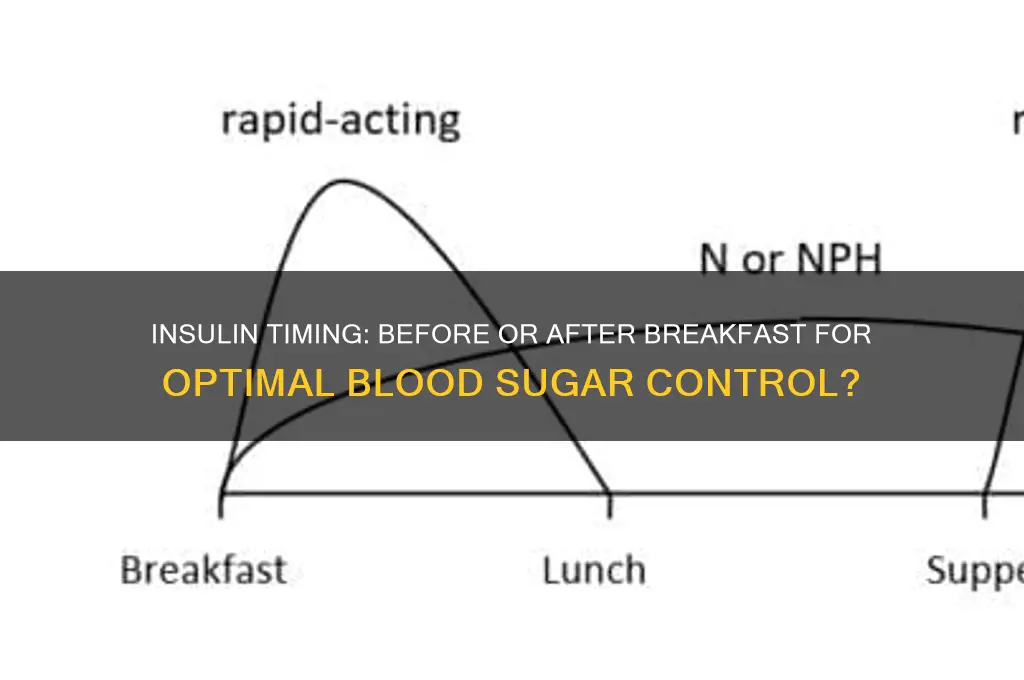
The timing of insulin administration in relation to meals, particularly breakfast, is a critical aspect of diabetes management that can significantly impact blood sugar control. Whether insulin should be given before or after breakfast depends on several factors, including the type of insulin used, the individual’s blood glucose levels, and their specific dietary habits. Rapid-acting insulin, for instance, is typically administered 15 to 20 minutes before a meal to allow it to start working as food is consumed, helping to prevent post-meal spikes in blood sugar. On the other hand, some individuals may opt to take insulin after breakfast if they are unsure of their meal size or composition, as this allows for more accurate dosing based on actual carbohydrate intake. Consulting a healthcare provider is essential to determine the most effective timing tailored to one’s unique needs and lifestyle.
| Characteristics | Values |
|---|---|
| Timing of Insulin Administration | Generally recommended to administer rapid-acting insulin 10-15 minutes before starting breakfast to align with meal absorption. |
| Type of Insulin | Applies primarily to rapid-acting insulin analogs (e.g., lispro, aspart, glulisine), which act quickly to manage post-meal glucose spikes. |
| Individual Variability | Timing may vary based on individual metabolism, type of meal, and specific insulin formulation. Consultation with a healthcare provider is essential. |
| Pre-Meal Blood Sugar Check | Recommended to check blood glucose before administering insulin to adjust dosage if needed. |
| Post-Meal Monitoring | Blood sugar should be monitored 2 hours after meals to assess insulin effectiveness and adjust future dosing. |
| Hypoglycemia Risk | Delaying insulin until after the meal increases the risk of post-meal hyperglycemia; taking it beforehand reduces this risk but requires careful timing to avoid hypoglycemia. |
| Meal Composition | High-carbohydrate or high-fat meals may require earlier insulin administration, while smaller meals may allow for more flexibility. |
| Clinical Guidelines | Most diabetes associations (e.g., ADA, EASD) recommend pre-meal dosing for rapid-acting insulin to optimize glycemic control. |
| Patient Education | Patients should be educated on the importance of consistent timing and coordination with meals to avoid complications. |
| Alternative Regimens | Some individuals may use pre-meal bolus calculators or insulin pumps for more precise timing and dosing. |
Explore related products





What You'll Learn
![]()
Timing Impact on Blood Sugar Control
The timing of insulin administration relative to meals, particularly breakfast, plays a crucial role in blood sugar control. When insulin is taken before breakfast, it allows the hormone to start lowering blood glucose levels in anticipation of the incoming carbohydrates. This proactive approach can prevent post-meal spikes, especially in individuals with rapid carbohydrate absorption. For those using rapid-acting insulin analogs, administering the dose 10-15 minutes before eating aligns the insulin peak activity with the rise in blood sugar from the meal, promoting better glycemic control. However, this timing requires careful planning to avoid hypoglycemia if the meal is delayed.
On the other hand, taking insulin after breakfast may be considered in certain scenarios, such as when the meal’s carbohydrate content is uncertain or when using regular insulin, which has a slower onset of action. This approach allows individuals to assess their meal intake and adjust the insulin dose accordingly, reducing the risk of over- or under-dosing. However, this method can lead to higher post-meal blood sugar levels, as insulin is not present to counteract the initial glucose surge. For optimal control, individuals must monitor their blood sugar closely and time their insulin dose to minimize this lag.
The impact of timing on blood sugar control is particularly significant for individuals with type 1 diabetes or insulin-dependent type 2 diabetes. Consistency in timing is key, as irregular administration can lead to unpredictable glucose fluctuations. For example, taking insulin before breakfast one day and after breakfast the next can disrupt the body’s ability to maintain stable blood sugar levels. Establishing a routine based on individual metabolism, insulin type, and lifestyle is essential for achieving long-term glycemic targets.
Another factor to consider is the type of breakfast consumed. High-carbohydrate meals require insulin to be timed more precisely to match the rapid glucose elevation. In contrast, protein-rich or high-fiber meals may allow for slightly more flexibility in timing, as they cause a slower and more gradual rise in blood sugar. Patients should work with healthcare providers to determine the best timing strategy based on their dietary habits and insulin regimen.
Ultimately, the goal of timing insulin around breakfast is to mimic the body’s natural response to meals as closely as possible. For most individuals, taking rapid-acting insulin before breakfast is recommended to optimize blood sugar control. However, personalized adjustments may be necessary based on factors like insulin type, meal composition, and individual response. Regular monitoring and collaboration with healthcare professionals are vital to fine-tune the timing and ensure effective management of blood glucose levels.
Choosing the Right Thickness for Your Breakfast Bar
You may want to see also
Explore related products




![Before and After [Blu-ray]](https://m.media-amazon.com/images/I/91u68VjjWWL._AC_UY218_.jpg)

![]()
Pre-Breakfast vs. Post-Breakfast Efficacy
The timing of insulin administration in relation to meals is a critical aspect of diabetes management, particularly for individuals with type 1 diabetes or insulin-dependent type 2 diabetes. The debate between administering insulin before or after breakfast centers on optimizing blood glucose control, minimizing postprandial spikes, and reducing the risk of hypoglycemia. Pre-breakfast insulin administration is often recommended because it allows the insulin to start acting as the meal is consumed, thereby mitigating the rapid rise in blood glucose levels that occurs after eating. This approach is especially beneficial for fast-acting insulin analogs, which have a quicker onset of action compared to regular insulin. By giving insulin 10–15 minutes before the meal, the peak activity of the insulin aligns more closely with the absorption of carbohydrates, leading to better glycemic control.
On the other hand, post-breakfast insulin administration may be considered in certain scenarios, such as when the carbohydrate content of the meal is uncertain or when there is a risk of skipping the meal. Administering insulin after eating allows for a more accurate assessment of the meal’s impact on blood glucose, enabling a more precise insulin dose. However, this approach carries a higher risk of postprandial hyperglycemia, as there is a delay between carbohydrate absorption and insulin action. For individuals using rapid-acting insulin, delaying the dose until after the meal may result in suboptimal control, as the insulin may not be able to counteract the rapid rise in blood glucose effectively.
Research comparing pre-breakfast and post-breakfast insulin administration has highlighted the advantages of the former. Studies have shown that pre-meal insulin dosing is associated with lower postprandial glucose excursions and improved HbA1c levels compared to post-meal dosing. This is particularly important for breakfast, as it is often the first meal of the day and sets the tone for glycemic control throughout the day. Additionally, pre-breakfast insulin administration aligns with the natural physiological response to meals, where endogenous insulin secretion begins in anticipation of food intake.
However, individual factors such as the type of insulin used, personal eating habits, and lifestyle must be considered when determining the optimal timing. For example, individuals using long-acting insulin or those with a history of hypoglycemia may require a more tailored approach. In such cases, consulting with a healthcare provider is essential to develop a personalized insulin regimen. It is also important to monitor blood glucose levels regularly to assess the effectiveness of the chosen timing and make adjustments as needed.
In conclusion, pre-breakfast insulin administration is generally more effective for achieving optimal glycemic control, as it allows insulin to counteract the rise in blood glucose from the meal more efficiently. While post-breakfast dosing may be appropriate in specific situations, it is less ideal for routine management due to the increased risk of hyperglycemia. Ultimately, the decision should be based on individual needs, the type of insulin used, and guidance from a healthcare professional. Consistent monitoring and adjustments are key to ensuring the chosen approach supports long-term diabetes management goals.
Is Breakfast at Tiffany's a Tale of a Call Girl?
You may want to see also
Explore related products






![]()
Risk of Hypoglycemia with Timing
The timing of insulin administration relative to breakfast is a critical factor in managing blood glucose levels and minimizing the risk of hypoglycemia. Hypoglycemia, or low blood sugar, occurs when glucose levels drop below the normal range, potentially leading to symptoms such as dizziness, confusion, and, in severe cases, loss of consciousness. The risk of hypoglycemia is particularly heightened when insulin is administered without proper consideration of meal timing. If insulin is given too early before breakfast, there is a longer gap between the insulin dose and food intake, which can cause blood sugar levels to drop excessively before the meal is consumed. This is especially true for rapid-acting insulin analogs, which begin to lower blood glucose within 15 minutes of injection.
Administering insulin immediately before or after breakfast can help mitigate this risk by ensuring that the insulin’s peak activity coincides with the rise in blood glucose from the meal. For example, taking rapid-acting insulin 10–15 minutes before eating allows it to start working as the meal is digested, reducing the likelihood of a significant drop in blood sugar. Conversely, delaying insulin administration until after the meal begins can also be effective, as it provides a more accurate assessment of carbohydrate intake and allows for adjustments based on actual food consumption. However, this approach requires careful monitoring to avoid post-meal hyperglycemia.
The risk of hypoglycemia is further influenced by individual factors such as metabolism, physical activity, and the type of insulin used. For instance, individuals with a faster metabolism or those who engage in morning exercise may experience a more rapid drop in blood sugar if insulin is given too early. Similarly, long-acting insulin, which has a more prolonged effect, may increase the risk of hypoglycemia if not balanced with timely meal consumption. Therefore, personalized timing strategies are essential to account for these variables and reduce the risk of hypoglycemic episodes.
Another consideration is the consistency of meal timing and insulin administration. Irregular eating patterns or delays in breakfast can disrupt the balance between insulin and glucose, increasing the risk of hypoglycemia. For example, if insulin is taken at the usual time but breakfast is significantly delayed, blood sugar levels may fall dangerously low. Establishing a routine where insulin is consistently taken either just before or just after breakfast can help maintain stable glucose levels and minimize the risk of hypoglycemic events.
In conclusion, the timing of insulin administration relative to breakfast plays a pivotal role in managing the risk of hypoglycemia. Taking insulin too early before the meal can lead to excessive glucose lowering, while administering it immediately before or after breakfast helps align insulin activity with food intake. Individual factors and consistent timing routines further influence this risk, emphasizing the need for personalized strategies. By carefully coordinating insulin timing with meal consumption, individuals can effectively reduce the likelihood of hypoglycemia and achieve better overall glucose control.
Perfectly Crispy Frozen Breakfast Potatoes: Easy Seasoning Tips & Tricks
You may want to see also
Explore related products





![]()
Individualized Insulin Timing Strategies
The timing of insulin administration relative to meals, particularly breakfast, is a critical aspect of diabetes management that requires personalization. Individualized Insulin Timing Strategies must account for factors such as the type of insulin used, the individual’s metabolism, lifestyle, and the composition of the meal. For instance, rapid-acting insulin analogs (e.g., lispro, aspart, glulisine) are typically recommended to be taken 10–15 minutes before a meal to align with the rise in blood glucose levels post-meal. However, this timing may vary based on the individual’s glycemic response and the speed of their carbohydrate digestion. Some individuals may benefit from taking insulin immediately before eating or even after the meal if they are unsure of the meal’s carbohydrate content or if they tend to skip meals frequently.
Another key consideration in Individualized Insulin Timing Strategies is the type of breakfast consumed. High-carbohydrate meals cause a rapid spike in blood glucose, necessitating insulin administration beforehand to prevent hyperglycemia. Conversely, a high-protein or high-fat breakfast may delay carbohydrate absorption, potentially requiring insulin to be taken slightly later. For example, a person eating oatmeal with fruit may need to take insulin 10–15 minutes prior, while someone having a breakfast rich in fats and proteins might benefit from a slightly delayed injection. Continuous glucose monitoring (CGM) can be invaluable in tailoring this timing by providing real-time data on how different meals and insulin schedules affect blood glucose levels.
Lifestyle factors also play a significant role in Individualized Insulin Timing Strategies. Individuals with irregular eating schedules or those who engage in morning physical activity may need to adjust their insulin timing accordingly. Exercise can increase insulin sensitivity and lower blood glucose levels, potentially requiring a reduction in the insulin dose or a delay in administration. Similarly, individuals who experience the "dawn phenomenon" (elevated morning blood glucose due to hormonal changes) may need to take their insulin earlier or use a basal insulin regimen to address this issue. Collaborating with a healthcare provider to analyze patterns and adjust timing based on lifestyle is essential for optimal control.
The role of patient education and self-monitoring cannot be overstated in Individualized Insulin Timing Strategies. Patients must understand how different factors—such as meal size, composition, and timing—impact their blood glucose levels. Regular self-monitoring of blood glucose (SMBG) or the use of CGM systems allows individuals to observe how their body responds to insulin and meals, enabling them to fine-tune their timing. For example, if post-breakfast blood glucose levels consistently rise too high, the insulin dose or timing may need adjustment. Empowering patients with knowledge and tools to make informed decisions is crucial for achieving personalized and effective insulin management.
Finally, Individualized Insulin Timing Strategies should be flexible and adaptable over time. Factors such as weight changes, aging, or shifts in physical activity levels can alter insulin sensitivity and meal responses, requiring periodic reassessment of timing. Regular follow-ups with healthcare providers, including endocrinologists or certified diabetes educators, are essential to review progress and make necessary adjustments. By adopting a dynamic and personalized approach to insulin timing, individuals with diabetes can achieve better glycemic control, reduce the risk of complications, and improve their overall quality of life.
Mastering the Art of Making Starbucks-Style Breakfast Sandwiches at Home
You may want to see also
Explore related products


![]()
Effect on Post-Meal Glucose Spikes
The timing of insulin administration in relation to meals, particularly breakfast, plays a crucial role in managing post-meal glucose spikes. When insulin is given before breakfast, it allows the hormone to start working as soon as carbohydrates from the meal are absorbed. This proactive approach helps to mitigate the rapid rise in blood glucose levels that typically occurs after eating. By priming the body with insulin, the liver and muscles become more receptive to glucose uptake, reducing the likelihood of a sharp spike. This method is particularly effective for individuals using rapid-acting insulin analogs, which begin to work within 15 minutes of injection.
Conversely, administering insulin after breakfast can lead to a delayed response, often resulting in higher post-meal glucose spikes. Since insulin takes time to reach its peak effect, the body may struggle to manage the influx of glucose from the meal, especially if it is carbohydrate-rich. This delay can cause blood sugar levels to rise significantly before the insulin takes effect, increasing the risk of hyperglycemia. For individuals with type 1 diabetes or insulin-dependent type 2 diabetes, this approach may require careful monitoring and adjustments to prevent prolonged high glucose levels.
The effect on post-meal glucose spikes is also influenced by the type of insulin used. Rapid-acting insulin, when given before breakfast, aligns closely with the meal’s digestion timeline, providing better control over glucose excursions. However, if given after the meal, its onset may not coincide with the peak glucose absorption, leading to suboptimal control. Intermediate or long-acting insulins, on the other hand, may not be as effective in preventing post-meal spikes regardless of timing, as they are designed for basal glucose management rather than meal coverage.
Individual factors, such as metabolism, meal composition, and insulin sensitivity, further impact the effect on post-meal glucose spikes. For instance, a high-carbohydrate breakfast requires insulin to be administered earlier to counteract the rapid glucose release. Similarly, individuals with slower gastric emptying may benefit from pre-meal insulin dosing to ensure the hormone is active when glucose enters the bloodstream. Personalized timing, based on these factors, is essential for minimizing post-meal spikes and maintaining overall glycemic control.
In conclusion, the timing of insulin administration significantly influences post-meal glucose spikes, with pre-breakfast dosing generally offering better control compared to post-meal dosing. This approach ensures that insulin is active during the critical period of glucose absorption, reducing the risk of hyperglycemia. However, individual variability and insulin type must be considered to optimize timing and achieve optimal glycemic outcomes. Consulting a healthcare provider to tailor insulin timing to specific needs is crucial for effective diabetes management.
German Breakfast Traditions: What's on the Morning Menu?
You may want to see also
Frequently asked questions
Insulin is typically given before breakfast, usually 10–15 minutes prior to eating, to help manage blood sugar spikes from the meal.
Giving insulin after breakfast is generally not recommended, as it may lead to higher post-meal blood sugar levels. Always follow your healthcare provider’s instructions.
Wait 10–15 minutes after injecting insulin before eating breakfast to ensure it starts working as the meal is digested.
Taking insulin after eating may result in delayed blood sugar control, increasing the risk of hyperglycemia (high blood sugar). Consult your doctor if this occurs.



















